

























Gonarthrosis of the knee joint is the most common localization of degenerative-dystrophic disease, characterized by the gradual destruction of cartilage with subsequent changes in the articular surfaces, accompanied by pain and decreased mobility.

The disease mainly affects women over 40 years of age, especially women who are overweight and have varicose veins of the lower extremities.
The knee joint consists of three sections:
- medial tibiofemoral;
- lateral tibiofemoral;
- suprapatellar-femoral.
These sections can be affected by deforming osteoarthritis (DOA) both individually and in any combination. 75% of all cases of gonarthrosis are the destruction of the tibiofemoral medial unit (during exercise there is a load that exceeds the body weight by 2-3 times).
In young patients, only one joint is destroyed more often - right or left (right-sided or left-sided gonarthrosis).
Causes of DOA of the knee joint
Several factors may be involved in the development of degenerative cartilage changes at the same time:
- mechanical loading of the knee joint with cartilage microtrauma (some specialties, sports);
- consequences of injuries, surgical interventions (menisectomy);
- inflammatory diseases of the knee (arthritis);
- anatomical inconsistencies of articular surfaces (dysplasia);
- violation of statics (straight legs, curvature of the spine);
- chronic hemarthrosis (accumulation of blood in the synovial cavity);
- metabolic pathologies (gout, hemochromatosis, chondrocalcinosis);
- excess body weight;
- disruption of blood supply to the bone;
- osteodystrophy (Paget's disease);
- neurological diseases, loss of sensation in the limbs;
- endocrine disorders (acromegaly, diabetes mellitus, amenorrhea, hyperparathyroidism);
- genetic predisposition (generalized forms of osteoarthritis);
- Disruption of type II collagen synthesis.
However, in 40% of cases it is impossible to determine the root cause of the disease (primary osteoarthritis).
Pathogenesis of gonarthrosis
initial stage
In the early stages of the disease, cartilage metabolism is disrupted. The synthesis and quality of proteoglycans, which are responsible for the stability of the structure of the collagen network, the main structural unit of cartilage tissue, decreases.
As a result, chondroitin sulfate, keratin, hyaluronic acid are washed from the mesh, and structurally defective proteoglycans can no longer retain water. Swollen fibers are absorbed into collagen, which reduces the resistance of cartilage to stress.
Anti-inflammatory substances accumulate in the synovial cavity, under the influence of which cartilage is destroyed even more rapidly. Fibrosis of the articular capsule develops. Changes in the composition of synovial fluid make it difficult for nutrients to reach the cartilage and disrupt the sliding of articular surfaces during movement.
Development of pathology
In the future, the cartilage gradually becomes thinner, rougher, and cracks appear along its entire thickness. The epiphyses of the bones are under increasing load, which leads to the development of osteosclerosis and compensatory proliferation of bone tissue (osteophytes).
This reaction of the body is aimed at increasing the area of articular surfaces and redistributing the load. However, the presence of osteophytes increases anxiety, deformity, and further limits joint mobility.
Micro-fractures occur in the thickness of the bone, which damages the blood vessels and causes intraosseous hypertension. In the final stage of osteoarthritis, the articular surfaces are completely exposed, deformed, and the movement of the limbs is severely limited.
Symptoms of gonarthrosis of the knee joint
Osteoarthritis of the knee joint is characterized by a chronic, slowly progressive course (months, years). The clinic grows gradually without acute exacerbations. The patient cannot remember exactly when the first symptoms appeared.
Clinical manifestations of gonarthrosis:
- pain. Initially diffuse, short (standing for a long time, climbing stairs) and as the osteoarthritis progresses, the pain becomes local (anterior and inner surface of the knee), their intensity increases;
- local sensitivity to palpation. Mainly on the inside of the knee along the edge of the joint space;
- crunch. In stage I it may be inaudible, in stage II-III it accompanies all movements;
- increase in volume, deformation of the knee. As a result of the weakening of the lateral ligaments, a person develops an O-shaped configuration of the extremities (this is clearly seen in the photo);
- restriction of mobility. First there are difficulties with bending the knee, then - extension.
Causes of pain in DOA:
- mechanical friction of damaged articular surfaces;
- increased intraosseous pressure, venous obstruction;
- connection of synovitis;
- changes in periarticular tissues (elongation of the capsule, ligaments, tendons);
- thickening of the periosteum;
- dystrophic events in adjacent muscles;
- fibromyalgia;
- compression of nerve endings.
Unlike coxarthrosis, DOA in the knee may indicate a spontaneous regression of symptoms.
Clinical manifestations of gonarthrosis depending on the stage:
| Features | i scene | Phase II | Phase III |
|---|---|---|---|
| Pain | It is more common when the knees are short (standing for a long time, climbing stairs) | The medium disappears after a night's rest | It is pronounced, and even at night it is disturbing |
| Restriction of movement | Invisible | There is an extension limitation, a slight limitation | Persistent flexion-extensor contractures, lameness |
| crunchy | no | It is felt during palpation during movement | distant crisis |
| Deformation | Missing | Slight deviation of the axis of the limb forward, muscle depletion | Valgus or varus deformity. The joint is unstable, atrophy of the thigh muscles |
| X-ray image | Slight narrowing of the joint space, early signs of subchondral osteosclerosis | The joint space narrows by 50% or more, osteophytes appear | Almost complete absence of joint space, significant deformation and sclerosis of articular surfaces, areas of subchondral bone necrosis, osteoporosis |
A common complication of osteoarthritis of the knee joint is secondary reactive synovitis characterized by the following symptoms:
- increased pain;
- swelling;
- effusion into the synovial cavity;
- increase in skin temperature.
Less common and more dangerous complications include: joint blockage, osteonecrosis of the femoral condyle, subluxation of the patella, spontaneous hemarthrosis.
DOA diagnosis of the knee joint
The diagnosis of gonarthrosis is based on the patient's characteristic complaints, changes found during the examination and the results of additional examinations.
Prescribed to confirm osteoarthritis:
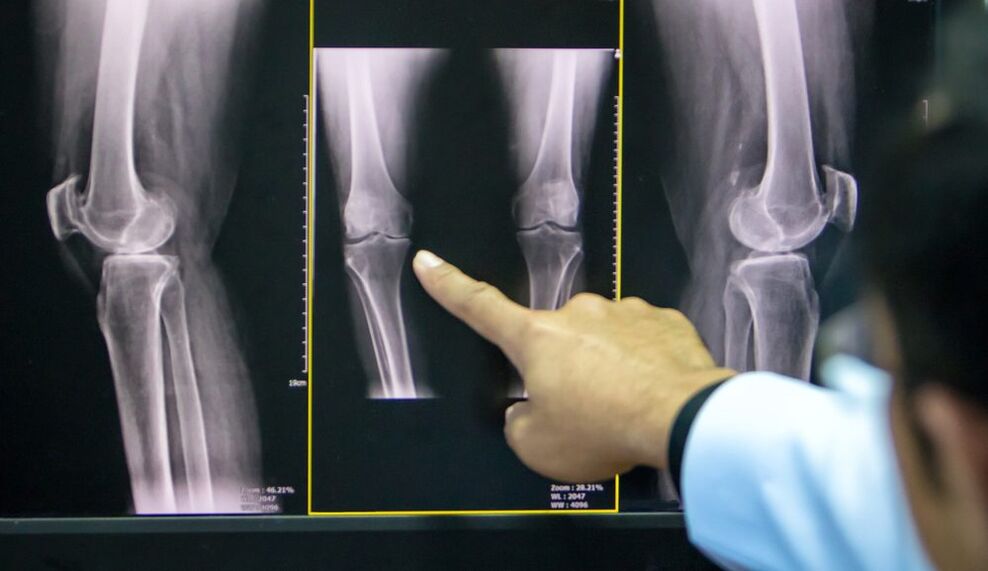
- X-ray of the knee joint in two projections (anteroposterior and lateral): the most accessible method to confirm the diagnosis at an advanced stage of pathology;
- Ultrasound: determination of the presence of effusion in the joint, measurement of cartilage thickness;
- analysis of synovial fluid;
- diagnostic arthroscopy with biopsy (visual assessment of cartilage);
- Computed tomography and magnetic resonance imaging (CT, MRI): the best method for the diagnosis of DOA in the early stages.
If the doctor has doubts about the diagnosis, it can be determined:
- scintigraphy: scanning of a compound after the introduction of a radioactive isotope;
- thermography: the study of the intensity of infrared radiation (its intensity is directly proportional to the intensity of inflammation).
Treatment of gonarthrosis of the knee joint
The treatment regimen for osteoarthritis combines several approaches: non-pharmacological methods, pharmacotherapy and surgical correction. The ratio of each method is determined individually for each patient.
Non-drug treatment
In the latest ESCEO (European Society of Clinical Aspects of Osteoporosis and Osteoarthritis) guidelines on how to treat knee osteoarthritis, experts pay special attention to patient education and lifestyle changes.

The patient needs:
- explain the nature of the disease established for long-term treatment;
- to teach to use auxiliary means (cane, orthosis);
- set a diet (for patients with a body mass index greater than 30);
- give a series of exercises to strengthen the thigh muscles and relax the knee joint;
- Explain the importance of increasing physical activity.
Physiotherapy methods of treatment in the early stages of osteoarthritis of the knee give good results:
- massage;
- magnetotherapy;
- UHF therapy;
- electrophoresis;
- hydrogen sulfide baths;
- paraffin applications;
- acupuncture.
Pharmacotherapy of gonarthrosis
The use of drugs in DOA aims to relieve pain, reduce inflammation and slow down the rate of cartilage destruction.
Symptomatic treatment:
- analgesics;
- non-steroidal anti-inflammatory drugs (NSAIDs) of the group of COX-2 inhibitors in tablet or suppository form;
- non-narcotic analgesics (with persistent pain syndrome).
Structural drugs (chondroprotectors):
- chondroitin sulfate;
- Glucosamine sulfate.
These drugs can be taken in the form of capsules in courses several times a year, injected intramuscularly or directly into the synovial cavity.
Topical therapy includes close and intraarticular injections of glucocorticosteroids, hyaluronic acid preparations.
An important part of complex therapy in stages I-II of DOA is the use of anti-inflammatory ointments, gels and creams based on NSAIDs. They help reduce the patient's need to take NSAIDs orally, thereby reducing the risk of damage to the digestive system.
Folk remedies
Tinctures, decoctions, extracts, topical applications of herbs should be considered as adjuvant methods for the treatment of DOA, folk remedies can not replace the therapy prescribed by a doctor.
Herbs used in osteoarthritis: ginger, artichoke, burdock, garlic, sea buckthorn.
Surgery
Inadequate medical intervention may require surgery at all stages of gonarthrosis. The most common are endoscopic procedures, in the most severe cases endoprosthesis replacement is indicated.

Types of endoscopic interventions:
- joint revision and rehabilitation: removal of inflammatory contents from the synovial cavity, cartilage fragments;
- plasma or laser ablation: removal of mechanical obstructions in the synovial cavity;
- chondroplasty.
Corrective periarticular osteotomy is indicated for patients with initial manifestations of axial deformity (not more than 15-20%).
The purpose of the operation is to restore the normal configuration of the joint, distribute the load evenly over the articular surface and remove the damaged areas. This procedure allows you to delay arthroplasty.
Tips for artificially replacing the affected area (or the entire joint):
- DOA II-III degree;
- severe axial deformation of the joint;
- aseptic necrosis of the subchondral bone layer;
- persistent pain syndrome.
Contraindications to knee arthroplasty:
- general joint damage;
- unstable garden apparatus;
- DOA as a result of inflammatory arthritis;
- persistent flexion contracture, severe muscle weakness.
In this case, the patient undergoes arthrodesis - a comparison of the removal of articular surfaces of the knee joint in the physiological state. This relieves pain, but shortens the leg, causing secondary injuries to the knee, hip and spine on the opposite side.
Prevention
Prevention of early cartilage degeneration should begin in childhood.
Precautions:
- prevention of scoliosis;
- correction of flat feet (shoes with arch supports);
- regular physical training (limit strenuous sports);
- exclusion of fixed postures during work.